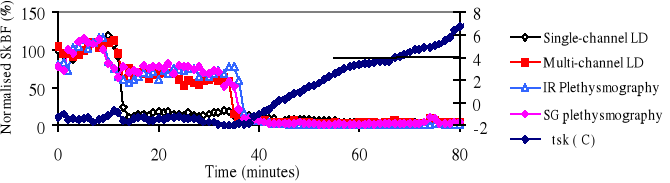
The forearm-finger pad skin temperature differential (Δtsk) has previously been used as an estimation of cutaneous skin blood flow (SkBF), vasoconstriction being considered significant when Δtsk Δ4°C (Sessler et al., 1988), on the basis that it “correlates well with other methods of determining cutaneous blood flow, including plethysmography”. The original source data (Goetz,, 1946) are from a study of SkBF (estimated by air-displacement plethysmography) and toe pad skin temperature only, not Δtsk. Goetz (1946) concluded that skin temperature starts rising only after SkBF has been increasing for some time. Thus, the Δtsk method would not seem to have been validated. This study was undertaken to assess if Δtsk can predict vasomotor tone as indicated by 4 other methods of estimating SkBF (House & Tipton, 2001). Δtsk was calculated from the difference between the radial mid-forearm skin temperature and that recorded from the index finger pad of the right hand. SkBF (4 techniques) was measured on the finger pads of the left hand which was immersed, without direct contact, in water at 38.5°C or 10.3°C, whilst the subjects were seated in a water bath heated initially to 40.6°C (House & Tipton, 2001). After ethical approval, seven medically fit volunteer subjects (6M 1F, aged 20-22 years) gave informed consent to participate. With heating, significant vasodilatation was indicated by all 4 methods, whilst Δtsk, was steady at -1.1°C (SD 0.6). When the left hand had been cooled, and the bath was being cooled [-0.6°C.min-1 (SD 0.2°C.min-1)], the 4 SkBF techniques simultaneously indicated profound vasoconstriction in 5 of the 7 subjects. At the corresponding time Δtsk started to increase approximately linearly. The response for subject 1 is shown in the figure. The point at which Δtsk started to rise, termed the “inflection point” of the response, defines the time of vasoconstriction more accurately than a particular value of Δtsk. For 4 subjects, the inflection point occurred simultaneously with vasoconstriction, as assessed by the other 4 methods. For the other 3 subjects, it occurred within 1 to 3 minutes. For 3 of the subjects, Δtsk only reached a maximum of 0.8°C to 2.7°C and, by the original criterion, would not have been regarded as indicating vasoconstriction, despite its occurrence. For 4 subjects, Δtsk reached 4°C 25 to 31 minutes after vasoconstriction, as identified by the other SkBF techniques. It is concluded that the Δtsk inflection point predicts cutaneous vasoconstriction better than Δtsk Δ4°C. The 4°C differential will confirm that vasoconstriction has occurred but not when, and not in all subjects.
Goetz, R.H. 1946. American Heart Journal. 31, 146-182.
House, J.R. and Tipton, M.J. 2001 Proc. APPS, 32(2) Suppl. 1, 58P.
Sessler, D.I., Olofsson, C.I., Rubinstein, E.H. 1988. Anethesiology 69, 357-364