Exercise induces myocytic potassium (K+) efflux, resulting in a large rise in circulating K+ concentration ([K+]), that is largely dependent upon both exercise intensity and the contracting muscle mass. K+ accumulation in muscle interstitial fluid has been linked to fatigue and performance decrements during exercise. Rowing involves intense contractions utilising a large proportion of the body's musculature. It was hypothesised that rowing at high intensity would cause a pronounced increase in circulating [K+] and muscle fatigue.
Eleven healthy, young adults (8 Male, 3 Female; age 24.73 ± 5.3 years, height 1.79 ± 0.09 m, mass 81.36 ± 12.2 kg, mean ± SD) performed a maximal 2000 m trial on a rowing ergometer. All participants were recreationally active, had rowing experience (on-water or gymnasium) and included four well trained rowers. Radial arterial blood samples were drawn at −10 min, on the rowing ergometer immediately pre-exercise (0 min), every 30 s during exercise and at 1, 2, 5, 10, 20 and 30 min post-exercise and analysed for fluid shifts, plasma electrolytes and acid-base status. Instantaneous rowing power output was recorded every 30 s and cardiorespiratory data were collected continuously during the trial.
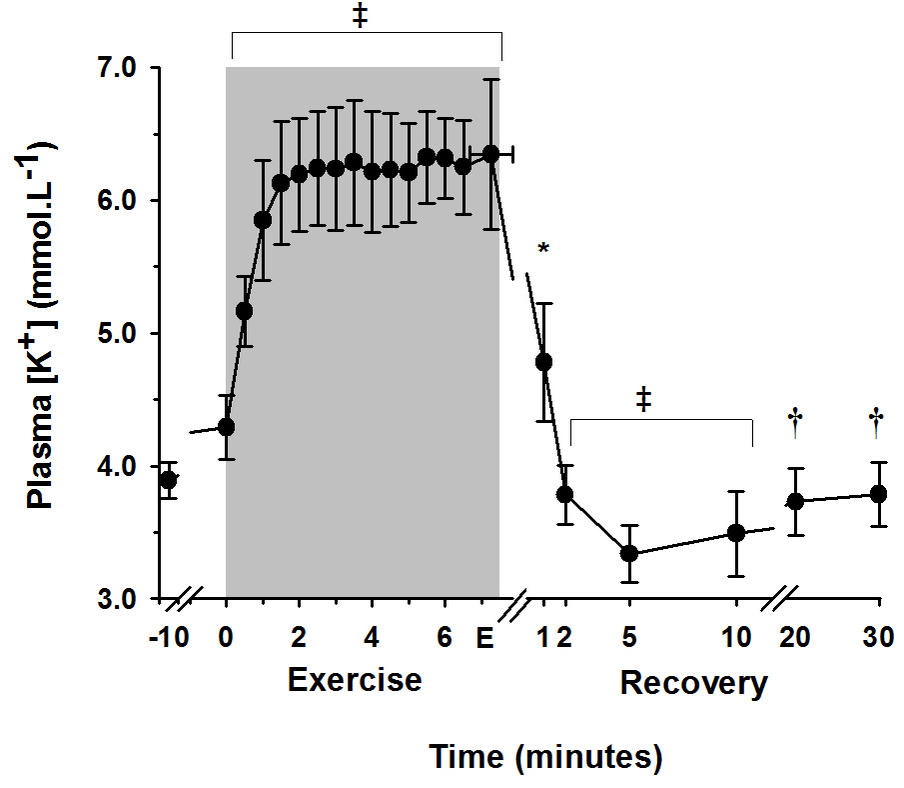
The time to complete 2000 m was 7.26 ±0.59 min. Power output was 326 ± 81 W in the first 30 s, tended to decline slightly until 4 min and remained unchanged until the end of exercise. At end-exercise, pulmonary oxygen uptake increased to 4.27 ±0.76 L.min−1, ventilation to 121.2 ±26.7 L.min-1 and heart rate to 177.0 ±9.8 beats.min−1. Arterial [K+] (Figure) was 3.89 ±0.13 mM at rest, rose slightly at pre-exercise (p < 0.005), increased to 6.13 ± 0.46 mmol.L−l after only 90 s exercise (p < 0.001) and remained unchanged thereafter for the rest of exercise (p < 0.001). Following exercise, plasma [K+] decreased abruptly to reach a nadir of 3.33 ± 0.22 mM at 5 min post-exercise (p < 0.001) and remained below pre-exercise levels at 30 min post-exercise (p < 0.005). Arterial [K+] was inversely correlated with power output (r= −0.50, p < 0.05). Plasma volume decreased from pre-exercise by 9.67 ± 2.29 % at end-exercise.
A high arterial [K+] was reached and sustained throughout the high intensity rowing trial. This elevation was not as great as anticipated, given the high intensity and large contracting muscle mass. These suggest that after 90 s of exercise, muscular Na+-K+-ATPase activity was sufficient to match muscle K+ release, thus minimizing an even more pronounced rise in extracellular [K+], in blood and most likely also in muscle.