Contents



|
|
Programme
Contents
|
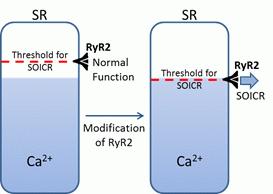
CPVT (catecholaminergic polymorphic ventricular tachycardia) is an inherited life-threatening arrhythmogenic disorder. CPVT is caused by DADs (delayed after-depolarizations) that are induced by spontaneous Ca2+ release during SR (sarcoplasmic reticulum) Ca2+ overload, a process also known as SOICR (store-overload-induced Ca2+ release). These Ca2+ release events occur through the cardiac ryanodine receptor (RyR2) with most instances of CPVT being attributed to mutations within RyR2. Using cytosolic and intra-SR Ca2+ imaging we have found that many of these CPVT-associated RyR2 mutations lead to SOICR by increasing the sensitivity of RyR2 to SR Ca2+, effectively reducing the SR Ca2+ load at which SOICR occurs (Jones et al., 2008) (see Figure). This is in keeping with the phenotype of CPVT where arrhythmias only occur during periods of stress, a condition known to increase SR Ca2+.
Subsequently, we and our collaborators have extended these studies and have found that sensitization of RyR2 to SR luminal Ca2+ activation represents a common mechanism of DADs and arrhythmia. To date we have shown that pro-arrhythmic drugs (Kong et al., 2008), phosphorylation of RyR2 (Xiao et al., 2007), and alterations in the macro-molecular complex surrounding RyR2 (Zhang et al., 2013) all result in sensitization of RyR2 to luminal Ca2+. However, not all SOICR events are created equal, as using a CPVT mutant mouse, that also has an altered SR Ca2+ store, we have recently demonstrated that frequent but small SOICR events do not lead to DADs and arrhythmia whereas scarcer but larger SOICR events almost always trigger DADs and arrhythmia (Bai et al., 2013). This suggests that both the occurrence and magnitude of SOICR events are important factors in determining whether arrhythmia will occur. Perhaps most excitingly, we have not only shown that the occurrence of SOICR is arrhythmogenic but that its inhibition is very effective at preventing CPVT mediated arrhythmia (Zhou et al., 2011). Given we have shown that aberrant regulation of RyR2 by multiple factors can trigger SOICR and arrhythmia, combining these data suggests that anti-SOICR agents targeting the threshold for store-overload-induced Ca2+ release may represent a new class of drugs for preventing many types of arrhythmogenic disorders.
Bai, Y., Jones, P. P., Guo J, Zhong X, Clark RB, Zhou Q, Wang R, Vallmitjana A, Benitez R, Hove-Madsen L, Semeniuk L, Guo A, Song LS, Duff HJ & Chen SR. (2013) Circulation Research 113, 517-26.
Jones PP, Jiang D, Bolstad J, Hunt DJ, Zhang L, Demaurex N & Chen SR. (2008) Biochemical Journal 412, 171-78.
Kong H, Jones PP, Koop A, Zhang L, Duff HJ & Chen SR. (2008) Biochemical Journal 414, 441-52.
Xiao B, Tian X, Xie W, Jones PP, Cai S, Wang X, Jiang D, Kong H, Zhang L, Chen K, Walsh MP, Cheng H & Chen SR. (2007) The Journal of Biological Chemistry 282, 30256-64.
Zhang J, McLay JM & Jones PP. (2013> Heart, Lung and Circulation 22, S78.
Zhou Q, Xiao J, Jiang D, Wang R, Vembaiyan K, Wang A, Smith CD, Xie C, Chen W, Zhang J, Tian X, Jones PP, Zhong X, Guo A, Chen H, Zhang L, Zhu W, Yang D, Li X, Chen J, Gillis A M, Duff HJ, Cheng H, Feldman AM, Song LS, Fill M, Back TG & Chen SR. (2011) Nature Medicine, 17, 1003-09.