Intense exercise causes pronounced increases in plasma potassium (K+), and often results in transient hypokalaemia during recovery. Skeletal muscle Na+,K+-ATPase plays a essential role in maintaining potassium homeostasis. Salbutamol has an stimulatory effect on skeletal muscle Na+,K+-ATPase and may thus affect potassium dynamics during exercise and in recovery. We investigated whether salbutamol lowered arterial plasma K+ concentration ([K+]a) during intense exercise and in recovery. Radial plasma [K+]a was measured during intense rowing exercise for 3 min in 11 healthy adults (age 30.6 ± 6.5 yr, height 1.81 ± 0.72 m, body mass 86.17 ± 10.90 kg, mean±SD) in a single-blinded randomised trial, either with or without 1000 μg salbutamol inhalation. Blood was sampled at baseline, during rowing exercise and for 60 min post-exercise and analysed for [K+], other electrolytes and acid-base.
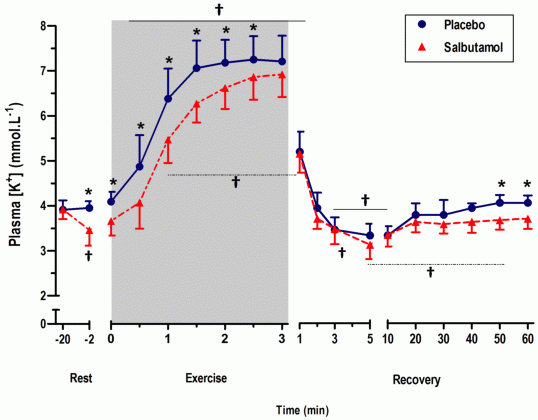
Plasma [K+]a revealed significant effects for time and condition (salbutamol) and time by condition interaction (P < 0.05). Arterial [K+] increased during exercise from baseline (-20 min) and pre-exercise (−2 min) reaching 7.06 ±0.61 mM at end exercise in placebo. In recovery, plasma [K+]a decreased rapidly, falling below baseline (P < 0.01) and pre-exercise (P < 0.001) by 3 min. Salbutamol lowered plasma [K+]a at rest by 0.45 mM and was increased to 6.92 ± 0.50 mM at end exercise in salbutamol (P < 0.05, The Figure). Following exercise plasma [K+]a reached a nadir of 3.06 ± 0.31 mM by 3 min (P < 0.05) in salbutamol. In recovery, salbutamol inhalation did not further lower plasma [K+]a immediately following exercise. At end-exercise, blood [lactate]a reached 12.52 ± 1.62 mM (placebo) and 11.99 ± 1.96 mM (salbutamol) (P < 0.05), pHa decreased to 7.13 ± 0.07 (placebo) and 7.16 ± 0.07 (salbutamol) (P < 0.05).
The pronounced and sustained arterial [K+] during rowing reflects the high intensity exercise and large contracting muscle mass with the post-exercise decline in plasma [K+]a to below baseline during recovery, likely due to continued Na+,K+-ATPase activity (Atanasovska, 2014). The lowering effect of plasma [K+]a with salbutamol likely reflects increased skeletal muscle Na+-K+-ATPase activity due to beta-agonist stimulation, but this was not more pronounced immediately following exercise with salbutamol. This suggests no additive effects of salbutamol beyond normal exercise induced plasma K+ lowering which may be a protective mechanism to prevent plasma [K+]a falling to dangerous levels.
Atanasovska T, Petersen AC, Rouffet DM, Billaut F, Ng I, McKenna MJ. (2014) Plasma K+ dynamics and implications during and following intense rowing exercise. Journal of Applied Physiology 117, 60-68.